Bioequivalence Explained: FDA Requirements to Prove Generic Equivalence

Have you ever wondered why your doctor prescribes a brand-name drug one month and a generic version the next? Or perhaps you’ve heard the rumor that generic medications are "weaker" because they aren't identical to the original. The truth is far more rigorous than those myths suggest. Behind every generic pill approved in the United States lies a strict scientific process called bioequivalence, defined by the absence of significant difference in the rate and extent of active ingredient absorption compared to the reference listed drug. This standard ensures that when you switch from a branded medication to its generic counterpart, your body receives the same therapeutic effect with no change in safety.
The U.S. Food and Drug Administration (FDA) doesn’t just guess that generics work; it demands proof. This proof comes through specific regulatory pathways established decades ago, ensuring that while the manufacturer changes, the clinical outcome remains exactly the same. Understanding these requirements demystifies how generic drugs save the healthcare system billions while maintaining high standards of care.
The Legal Foundation: Hatch-Waxman and ANDAs
To understand bioequivalence, we first need to look at the legal framework that allows generic drugs to exist. Before 1984, pharmaceutical companies held monopolies on their drugs for long periods after patents expired, keeping prices artificially high. That changed with the Drug Price Competition and Patent Term Restoration Act of 1984, commonly known as the Hatch-Waxman Act.
This legislation created a streamlined approval pathway called the Abbreviated New Drug Application (ANDA). Unlike a full New Drug Application (NDA) required for brand-new medicines, an ANDA does not require the generic manufacturer to repeat costly and time-consuming preclinical animal studies or large-scale human clinical trials. Instead, the manufacturer must prove two things:
- Pharmaceutical Equivalence: The generic contains the same active ingredient, in the same strength, dosage form, and route of administration as the brand-name drug.
- Bioequivalence: The generic performs in the body in the same way as the brand-name drug.
The logic here is efficient and scientifically sound. If the chemical structure is identical and the body absorbs it identically, the clinical results will be identical. This bridge between the brand-name data and the generic product is what makes the modern generic market possible.
How Bioequivalence Is Measured: Cmax and AUC
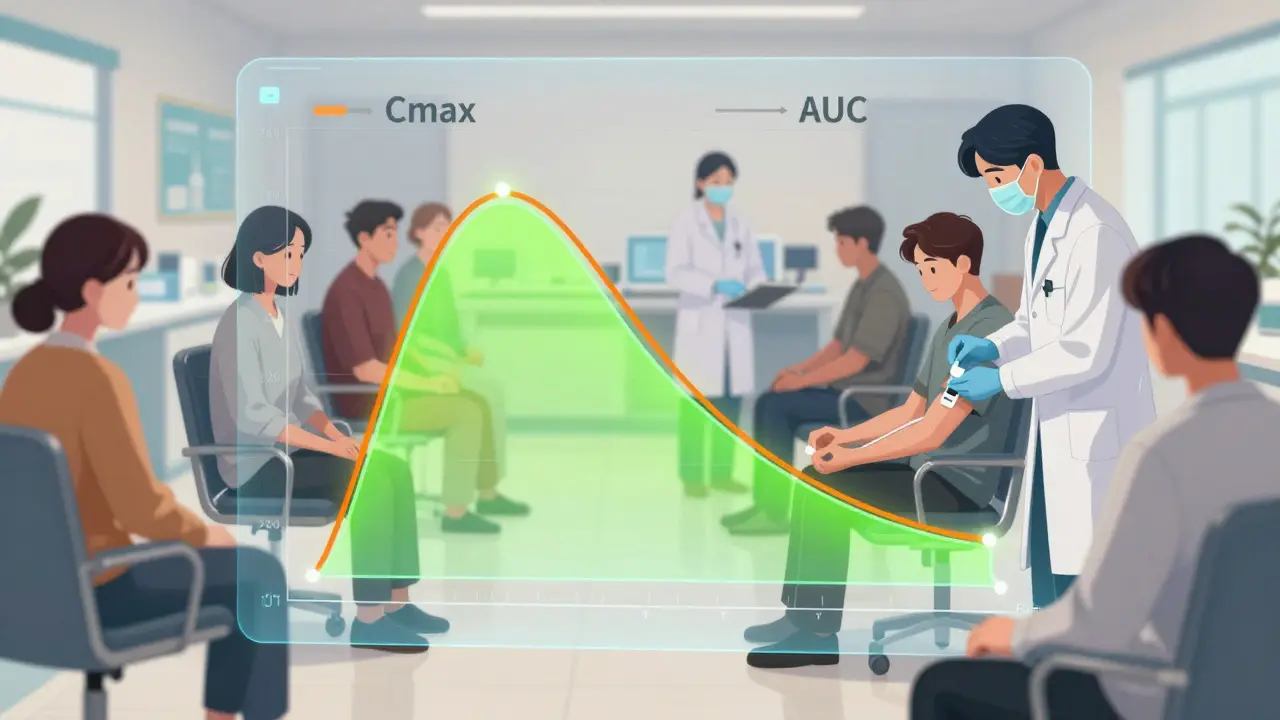
So, how do regulators actually measure if a drug behaves the same way? They don’t test every patient in the world. Instead, they conduct randomized crossover trials, typically involving 24 to 36 healthy volunteers. These studies focus on pharmacokinetic (PK) parameters-essentially, what the body does to the drug.
Two key metrics determine success:
- Cmax (Peak Concentration): This measures the highest concentration of the drug in the bloodstream. It tells us how quickly the drug works. If a painkiller needs to act fast, Cmax is critical.
- AUC (Area Under the Curve): This represents the total amount of drug absorbed over time. It indicates the overall exposure to the medication. There are two types: AUC(0-t), which tracks absorption until the last measurable dose, and AUC(0-∞), which extrapolates to infinity to account for slow elimination.
For a generic drug to pass, its Cmax and AUC values must match those of the Reference Listed Drug (RLD), the original brand-name product against which all generics are compared.
The 80-125% Rule: Debunking the Myth
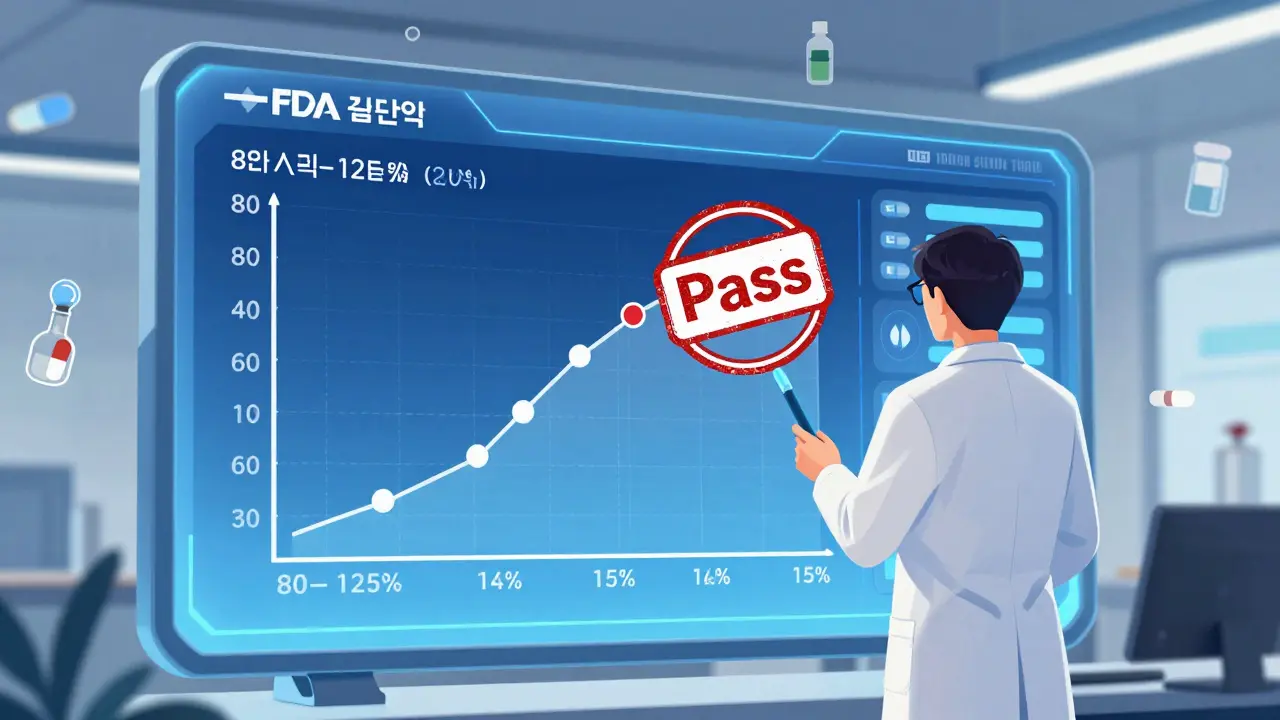
Here is where confusion often arises. You may have heard that generic drugs can contain anywhere from 80% to 125% of the active ingredient compared to the brand name. This is a dangerous misconception. The FDA requires the exact same amount of active ingredient in both products. The 80-125% range applies strictly to the pharmacokinetic parameters (Cmax and AUC), not the physical content of the pill.
The FDA requires that the 90% confidence interval (CI) of the ratio between the generic and the reference drug falls within the range of 80% to 125%. Let’s break down what that means with a concrete example.
Imagine a brand-name drug has an AUC of 100 units. A generic version is tested, and the observed mean AUC is 93 units. The statistical analysis calculates a 90% confidence interval of 84% to 110%. Since both the lower bound (84%) and the upper bound (110%) fall inside the 80-125% window, the drug passes.
Now, consider a failing case. If the mean ratio is 116%, but the 90% CI ranges from 103% to 130%, the drug fails. Why? Because the upper bound (130%) exceeds the permissible limit of 125%. This statistical rigor ensures that even in worst-case scenarios within the study population, the difference remains clinically insignificant.
| Metric | Brand-Name Value | Generic Mean Value | 90% Confidence Interval | Result |
|---|---|---|---|---|
| AUC Example 1 | 100% | 93% | 84% - 110% | Pass (Within 80-125%) |
| AUC Example 2 | 100% | 116% | 103% - 130% | Fail (Upper bound > 125%) |
| Cmax Example | 100% | 98% | 90% - 107% | Pass (Tight fit) |
Dr. Utpal Munshi, an expert in bioequivalence studies, emphasizes that this 20% difference threshold is statistically derived and considered clinically insignificant for most drugs. In other words, a small variation in blood levels does not translate to a noticeable difference in how well the drug treats your condition or its side effects.
In Vivo vs. In Vitro Testing Methods
Not all drugs are tested the same way. The FDA tailors its approach based on how the drug works in the body. The primary decision is whether to use in vivo (inside the living body) or in vitro (in a lab setting) testing.
In Vivo Studies are the gold standard for systemic drugs-medications intended to be absorbed into the bloodstream and distributed throughout the body. Examples include oral tablets for hypertension or antibiotics. These require the crossover trials mentioned earlier, measuring blood concentrations over time.
In Vitro Studies are often sufficient for locally acting drugs. Think of topical creams for eczema, nasal sprays for allergies, or eye drops. Since these drugs are not meant to enter the bloodstream significantly, measuring blood levels isn't useful. Instead, manufacturers test dissolution rates (how fast the drug dissolves) or conduct comparative clinical trials focusing on local efficacy, such as reducing redness or swelling.
The FDA publishes over 2,000 product-specific guidances to help manufacturers choose the right path. These documents detail whether a specific dosage form or route of delivery requires complex modeling or simple dissolution testing.
Narrow Therapeutic Index Drugs: Tighter Standards?
Some medications leave very little room for error. These are known as Narrow Therapeutic Index (NTI) drugs. For these drugs, a small change in blood concentration can lead to treatment failure or toxicity. Examples include warfarin (a blood thinner), levothyroxine (for thyroid conditions), and certain anti-seizure medications like phenytoin.
Historically, there was debate about whether NTI drugs should have tighter bioequivalence limits than the standard 80-125%. Some experts argued for a range of 90-111%. However, the FDA maintains that the standard 80-125% range is appropriate for most NTI drugs, provided the manufacturing process is highly controlled. The agency argues that the variability in how individual patients metabolize drugs is often greater than the variability allowed between the generic and brand-name versions. Therefore, switching brands rarely causes clinical issues if the bioequivalence standards are met.
Transparency and Future Trends
The landscape of generic drug approval is evolving toward greater transparency. Until recently, manufacturers only had to submit bioequivalence studies that demonstrated success. If a study failed, it could be omitted from the application. Starting in 2021, the FDA amended regulations to require ANDA applicants to submit data from all bioequivalence studies conducted on a formulation, regardless of the outcome. This change aims to give regulators and healthcare providers a complete picture of the drug's performance history.
Looking ahead, the FDA’s 2022-2026 strategic plan highlights the use of modeling and simulation. By using computer models to predict how a drug will behave, the agency hopes to reduce the need for some clinical bioequivalence studies, particularly for complex products like inhalers and transdermal patches. This innovation could speed up approvals while maintaining safety standards.
The impact of these rigorous standards is massive. Generic drugs account for approximately 90% of prescriptions filled in the United States but represent only about 20% of total drug spending. Over the decade from 2010 to 2019, this system saved the U.S. healthcare system an estimated $1.7 trillion. Without the strict bioequivalence requirements established by the FDA, this economic benefit would come at the cost of patient safety and trust.
What is the difference between pharmaceutical equivalence and bioequivalence?
Pharmaceutical equivalence means the generic and brand-name drugs contain the same active ingredient, in the same strength, dosage form, and route of administration. Bioequivalence goes further, proving that the body absorbs and processes the generic drug at the same rate and extent as the brand-name drug. Both are required for FDA approval via an ANDA.
Does the 80-125% rule mean generics have less medicine?
No. This is a common myth. The 80-125% range applies to the pharmacokinetic parameters (Cmax and AUC), specifically the 90% confidence interval of the ratio between the generic and brand-name drug. It does not refer to the actual amount of active ingredient in the pill, which must be identical.
Why do some doctors prefer brand-name drugs over generics?
While bioequivalence standards ensure clinical similarity, some physicians may prefer brand-name drugs for narrow therapeutic index medications due to personal experience or concerns about inactive ingredients (excipients). However, for the vast majority of drugs, generics are therapeutically equivalent and safer for patients financially.
How long does it take for the FDA to approve a generic drug?
The FDA review process for an Abbreviated New Drug Application (ANDA) typically takes 10 to 12 months for standard reviews. The first-cycle approval rate is around 65%, meaning many applications require additional information or reformulation before final approval.
Are bioequivalence studies done on patients or healthy volunteers?
Most bioequivalence studies are conducted on healthy volunteers rather than patients with the disease. This isolates the variable of drug absorption without the confounding factors of illness. Typically, these trials involve 24 to 36 participants in a randomized crossover design.