Antihistamines in Elderly Patients: Why Older Adults Face Higher Risks of Confusion and Falls
Elderly Antihistamine Risk Calculator
Select the factors that apply to the patient to calculate their estimated risk profile.
Risk Assessment
Select factors above to see specific medical guidance.
Imagine a 78-year-old woman sitting in her living room. She feels perfectly fine until she takes an over-the-counter sleep aid for a restless night. Within hours, she becomes disoriented, packs her bags to "go home," even though she is already there. This isn't a scene from a movie; it is a documented reality for many older adults taking common allergy or sleep medications. The culprit? First-generation antihistamines, specifically those with strong anticholinergic properties that affect the brain.
We often view these drugs as harmless household staples. Diphenhydramine (Benadryl) and doxylamine (Unisom) have been on shelves since the 1940s. But for anyone over 65, the body processes these chemicals differently. The result is not just drowsiness-it is a significant risk of acute confusion, dangerous falls, and long-term cognitive decline. Understanding why this happens is the first step in protecting yourself or your loved ones.
The Blood-Brain Barrier Breakdown
To understand the danger, you need to look at how these drugs move through the body. Histamine is a chemical your body releases during allergic reactions. Antihistamines block the receptors that histamine attaches to, stopping symptoms like itching or sneezing. However, there are two main types of these medications, and they behave very differently.
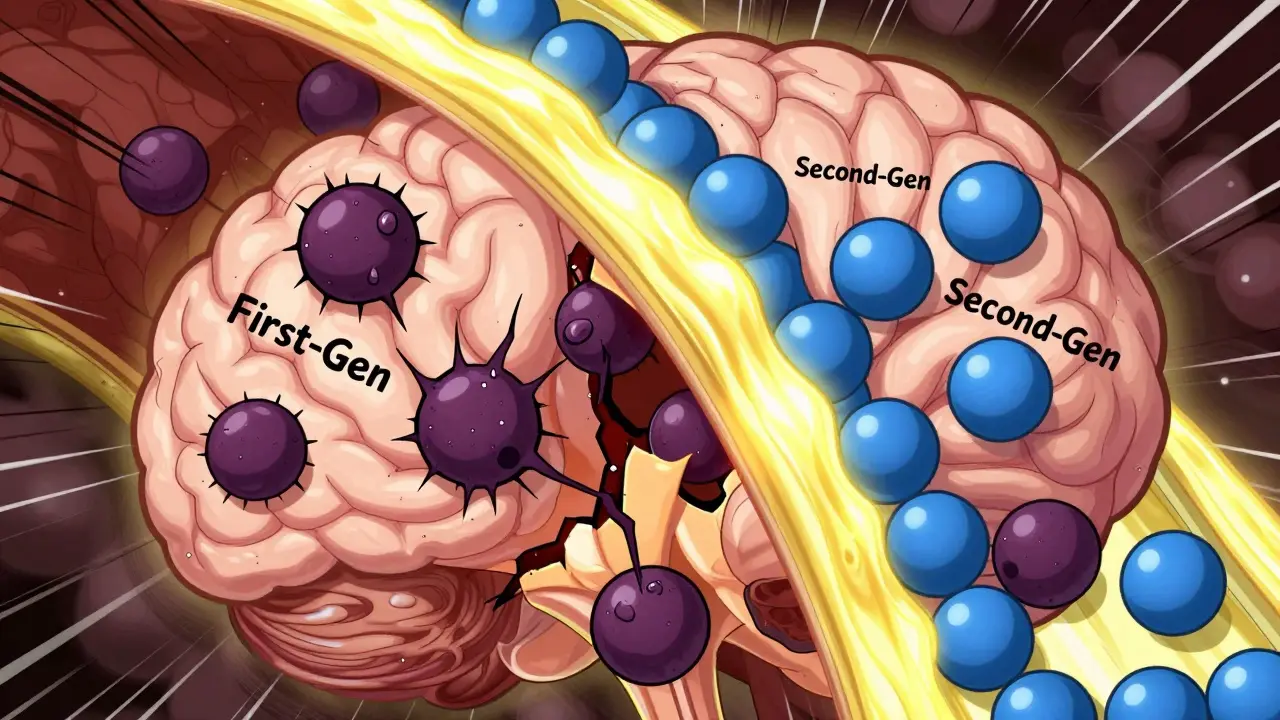
First-generation antihistamines, such as diphenhydramine, chlorpheniramine, and hydroxyzine, are lipophilic. In plain English, they love fat. Because the lining of your blood vessels and the barrier protecting your brain are made of fatty tissue, these drugs slip right through. They cross the blood-brain barrier easily, entering the central nervous system where they cause sedation and mental fog.
Second-generation antihistamines, including cetirizine (Zyrtec), loratadine (Claritin), and fexofenadine (Allegra), were engineered later to solve this exact problem. Their molecules are polar, meaning they do not pass easily through fatty barriers. They stay mostly in the peripheral tissues-like your nose and skin-where they treat allergies without messing with your brain chemistry. For an elderly patient, this distinction is life-changing.
Why Age Changes Everything
You might wonder why a younger person can take Benadryl and just feel sleepy, while an older adult ends up confused. The answer lies in natural aging processes. As we age, our bodies produce less acetylcholine, a neurotransmitter essential for memory, attention, and alertness.
Dr. Shelly Gray, a researcher specializing in aging and pharmacotherapy, explains that blocking the effects of acetylcholine delivers a "double whammy" to older people. First-generation antihistamines act as muscarinic receptor antagonists. They don't just block histamine; they also block acetylcholine. When you combine an age-related drop in acetylcholine with a drug that blocks what little remains, the result is profound cognitive impairment.
This leads to the classic signs of anticholinergic toxicity, often remembered by the medical mnemonic: "blind as a bat, dry as a bone, red as a beet, mad as a hatter, and hot as a hare." In elderly patients, this manifests as blurred vision, severe dry mouth, constipation, urinary retention, and agitation or delirium. It is not just a side effect; it is a physiological crisis.
The Hidden Danger of Falls
Cognitive confusion is scary, but physical injury is often the immediate consequence. Dizziness, hypotension (low blood pressure), and next-day sedation compromise balance and coordination. For seniors, a fall is never minor. It can lead to hip fractures, head trauma, and a loss of independence that permanently alters quality of life.
The data supports this concern starkly. A 2018 systematic review published in PubMed analyzed five observational studies involving elderly patients. The findings were clear: using first-generation antihistamines increased the risk of injurious falls or fractures by 103%. That means the odds ratio was 2.03 compared to non-users. To put that in perspective, if you take these drugs, you are more than twice as likely to suffer a serious fall-related injury.
| Feature | First-Generation (e.g., Benadryl) | Second-Generation (e.g., Claritin) |
|---|---|---|
| Blood-Brain Barrier Penetration | High (Crosses easily) | Low (Limited penetration) |
| Fall Risk Increase | 103% higher risk (OR 2.03) | Negligible association |
| Cognitive Side Effects | Confusion, delirium, dementia risk | Minimal to none |
| Peripheral Side Effects | Dry mouth, constipation, urinary retention | Rare |
| Sedation Level | Significant | Non-sedating (mostly) |
Long-Term Cognitive Consequences
The risks do not end when the medication wears off. There is growing evidence that chronic use of anticholinergic drugs contributes to long-term brain damage. A landmark study published in JAMA Internal Medicine in 2015 tracked participants for an average of seven years. Among 800 volunteers who developed dementia, those who had used anticholinergic medications showed a 54% higher risk compared to those who took equivalent doses for shorter periods.
This suggests a cumulative effect. Every time you block acetylcholine receptors, you may be accelerating neurodegenerative processes. For families caring for relatives with early-stage memory issues, continuing to prescribe or purchase first-generation antihistamines could be actively worsening the condition. The goal should always be to preserve cognitive reserve, not erode it.
Why Are These Drugs Still So Common?
If the science is so clear, why are 34.7% of adults aged 65+ still regularly using first-generation antihistamines? According to a 2023 study in the Journal of the American Geriatrics Society, nearly 18% use them daily. Several factors drive this persistence.
First, familiarity breeds trust. Many seniors grew up using these brands and associate them with relief. Second, marketing plays a huge role. Sales data from IQVIA shows diphenhydramine remains one of the top 20 over-the-counter purchases for Americans over 65, generating over $350 million annually. Third, hidden ingredients are everywhere. These drugs are not just in allergy pills; they are in "nighttime" pain relievers, cough syrups, and multi-symptom cold remedies. A senior might think they are buying simple acetaminophen, but they are actually ingesting a potent anticholinergic agent.
Regulatory bodies have tried to intervene. The American Geriatrics Society’s Beers Criteria, updated in 2019, explicitly lists first-generation antihistamines as "potentially inappropriate medications" for older adults. Centers for Medicare & Medicaid Services (CMS) now track anticholinergic use in nursing homes, penalizing facilities where more than 5% of residents receive high-risk meds. Yet, change is slow because consumer awareness lags behind clinical guidelines.

Safer Alternatives and Practical Steps
You do not have to live with allergies or insomnia. The key is switching strategies. Here is how to approach medication safety for elderly patients:
- Switch to Second-Generation Antihistamines: Loratadine (Claritin) at 10 mg daily or cetirizine (Zyrtec) at 5 mg daily are preferred options. Fexofenadine (Allegra) at 60 mg twice daily is another safe choice. These provide effective symptom relief without crossing into the brain.
- Review All Medications Quarterly: Conduct a comprehensive medication review every three months. Check every bottle, including over-the-counter items. Look for diphenhydramine or doxylamine in the active ingredients list.
- Use Non-Pharmacological Tools: For allergies, saline nasal sprays, HEPA air filters, and allergen-proof bedding can reduce symptoms without drugs. For sleep, focus on sleep hygiene: consistent schedules, reduced screen time before bed, and limiting caffeine.
- Watch for Drug Interactions: Antidepressants and other psychotropic drugs can exacerbate anticholinergic side effects. Always discuss new medications with a doctor or pharmacist to check for interactions.
If an elderly patient is currently experiencing confusion or delirium after taking an OTC sleep aid, stop the medication immediately. In many cases reported by geriatric nurses, acute confusion resolves within 72 hours of discontinuing the antihistamine. However, always consult a healthcare provider before making sudden changes to a medication regimen.
Conclusion: A Simple Swap for Better Safety
The transition from first-generation to second-generation antihistamines is one of the most impactful, low-cost interventions available in geriatric care today. Experts estimate that eliminating inappropriate use could prevent approximately 250,000 falls and 50,000 dementia cases annually in the United States alone. It is not about banning old medicines; it is about respecting how the aging body changes. By choosing safer alternatives and staying vigilant about hidden ingredients, you can protect cognitive health and physical safety without sacrificing comfort.
What are the most common signs of antihistamine toxicity in the elderly?
Common signs include acute confusion, disorientation, severe drowsiness, dry mouth, blurred vision, constipation, urinary retention, and agitation. In severe cases, it can lead to delirium or hallucinations. If you notice sudden behavioral changes after starting a new OTC medication, suspect anticholinergic toxicity.
Is Benadryl safe for seniors to use occasionally?
The American Geriatrics Society advises against using first-generation antihistamines like Benadryl (diphenhydramine) in older adults entirely, even occasionally. Due to the high risk of falls, confusion, and cognitive decline, safer second-generation alternatives like Claritin or Zyrtec are strongly recommended instead.
How long does it take for confusion caused by antihistamines to resolve?
In many cases of acute anticholinergic delirium, symptoms begin to improve within 24 to 72 hours after stopping the medication. However, full resolution depends on the individual's overall health, hydration status, and whether other contributing factors are present. Medical supervision is advised during this period.
Which second-generation antihistamines are best for older adults?
Loratadine (Claritin), cetirizine (Zyrtec), and fexofenadine (Allegra) are considered safe and effective for elderly patients. They do not cross the blood-brain barrier significantly, minimizing the risk of sedation and cognitive side effects. Always start with the lowest effective dose and consult a doctor for personalized advice.
Can antihistamines interact with other common medications?
Yes, first-generation antihistamines can interact dangerously with antidepressants, antipsychotics, and certain heart medications. These combinations can amplify anticholinergic effects, leading to increased confusion, rapid heartbeat, and severe constipation. A pharmacist can review your medication list for potential interactions.